
.avif)
Lateral knee pain (outside of the knee) is common in young athletes, active adults, sedentary adults and post surgical patients. Lateral knee pain has many different causes that may originate from musculoskeletal issues, changes in biomechanics, inflammation or degeneration, like arthritis. Lateral knee pain is a complex diagnosis since it can be caused by many, many different things such as the iliotibial band (IT band), lateral collateral ligament (LCL), the meniscus, the retinaculum of the quads, the biceps femoris. It can even be stemming from issues at the hip, low back and even the feet. We will discuss many details of these common areas in this article and dive into lateral knee pain after a knee replacement or with individuals with knee arthritis.
Anatomy of the lateral knee
There are many different structure of the outside of the knee that have different purposes:
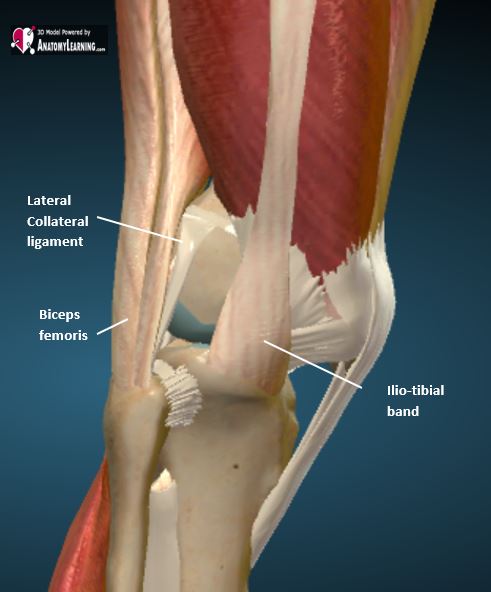
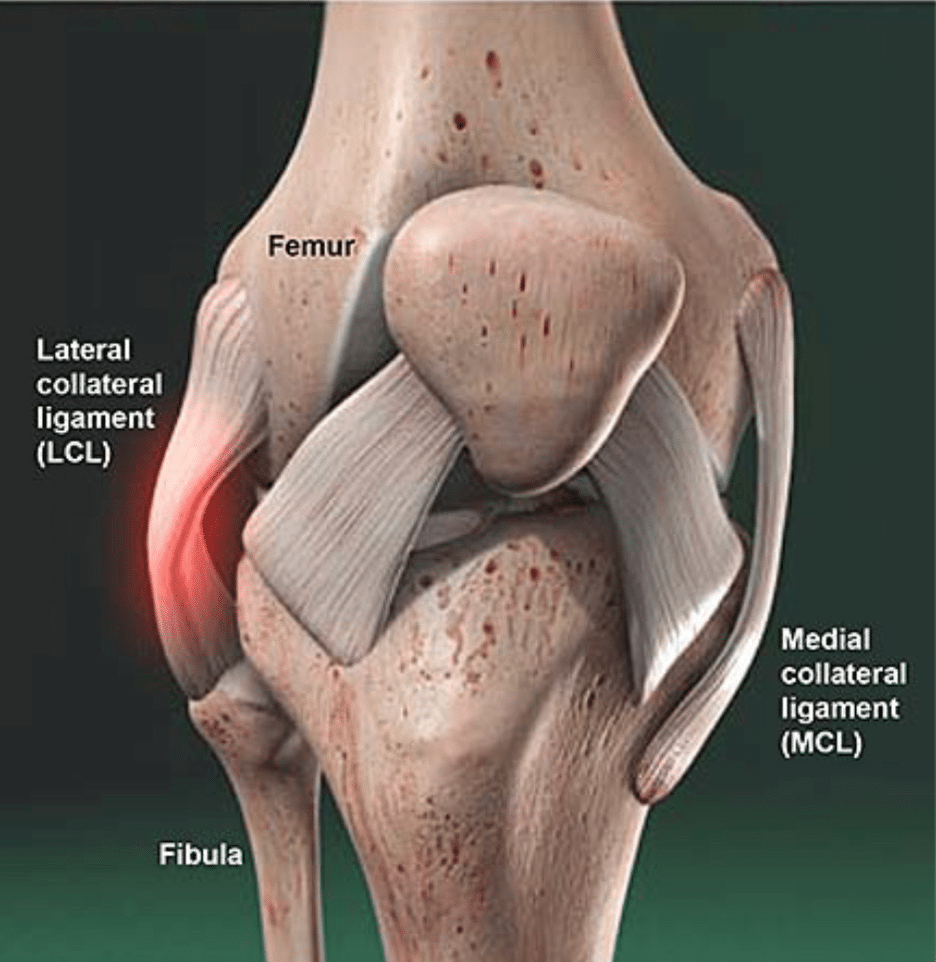
- Lateral Collateral Ligament (LCL): this ligament is attached from the outside of the femur to the head (top) of the fibula. It is a strong, rope-like structure that helps keep the knee from varus forces.
- Iliotibial Band (IT Band): this band is a thick band of connective fascial tissue that runs down the outside of the thigh and knee. The IT band originates on the outside of the hip on the TFL muscle and attaches on the outside of the femur. The IT band stabilizes the outside of the knee during movement.
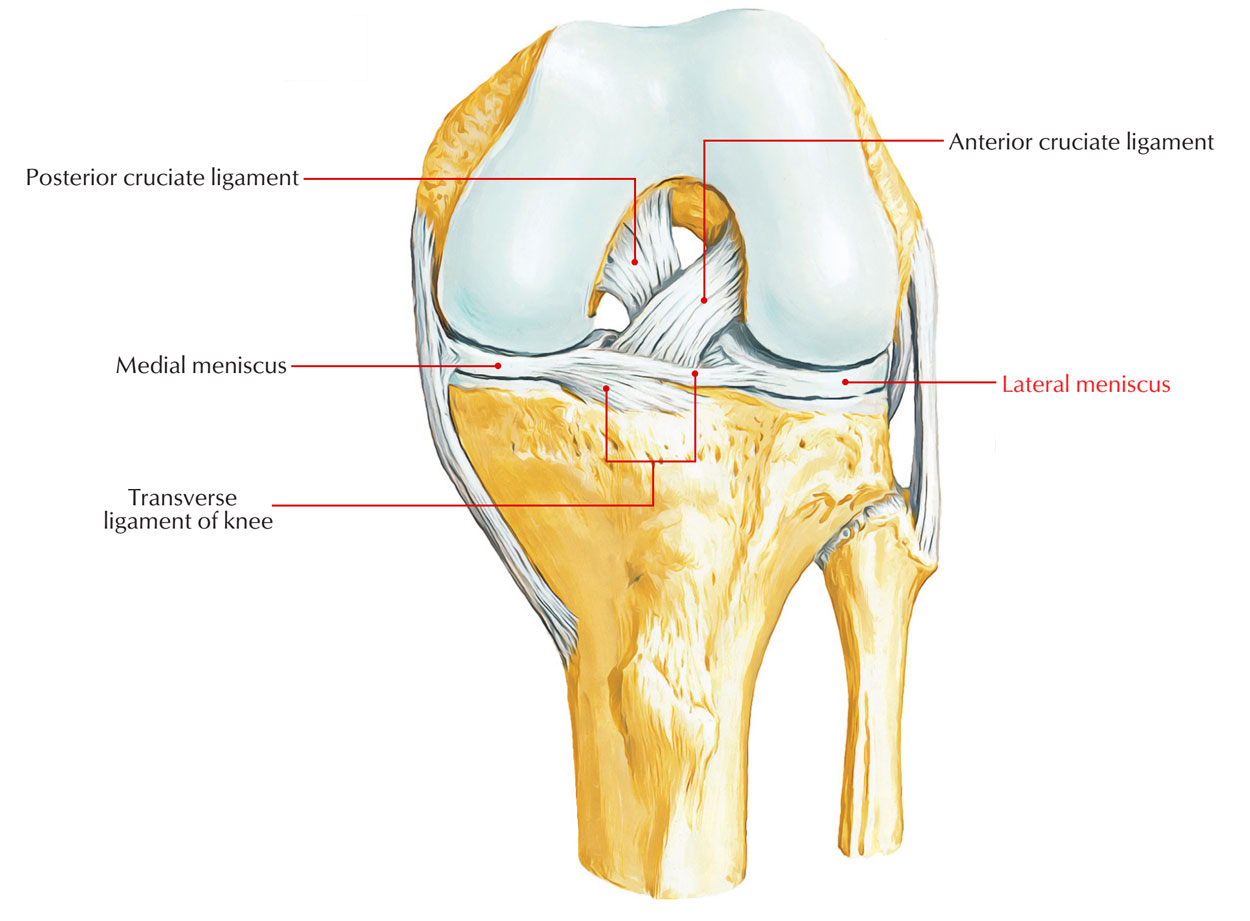
- Lateral meniscus: both the lateral and medial meniscus provide a cushion for the knee joint. The lateral meniscus is bigger and more moveable.
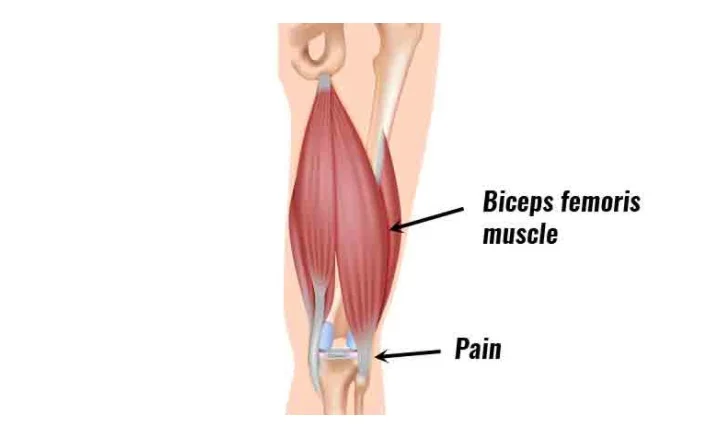
- Biceps Femoris Tendon: this is one of the hamstring tendons that provides stability to the outside of the knee. The tendon attaches to the head (top) of the fibula right by the LCL.
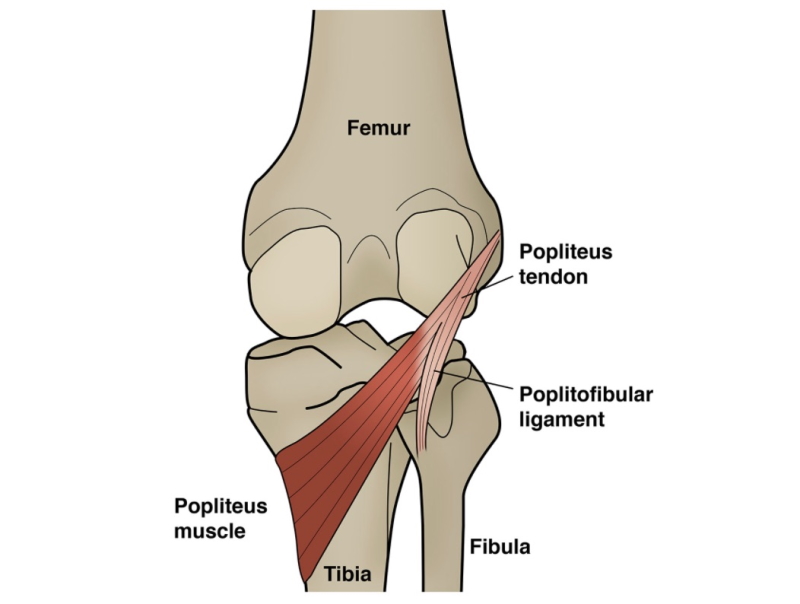
- Popliteus Tendon: this tendon stabilizes the side and back of the knee. The muscle also helps start the begin phases of knee bending after the knee is completely straight.
- Lateral Capsule: this is a fibrous envelope the surrounds the entire knee, but the lateral portion of the capsule does provide support and stability to the knee.
All of these structures can lead to lateral knee pain if there is some sort of dysfunction happening in the knee. Let's discuss these structures in detail.
Lateral Collateral Ligament (LCL) Injury
Typically, with LCL injuries, there is some sort of traumatic event that happens to the medial side of the knee or a sudden twist, during contact sports such as football, soccer or skiing. The LCL stretches and tears. The injury can be a mild stretch to a complete tear that would require surgery to fix. Another way the LCL is commonly overstretched or torn is with hyperextension (excessive straightening) to the knee. When the knee hyperextends beyond normal range, this can cause high tension on the outside portion of the knee where the LCL is. This happens in skiing or even landing incorrectly from a jump.
The LCL can also become chronically worn and irritated overtime if you have poor biomechanics of the knee. This is often seen in individuals with bow legs (genu varum). This can cause a lot of irritation over many years, which leads to an overstretched LCL. When the LCL is too "stretchy", then it cannot provide stability to the outside of the knee.
If you have had a knee replacement, 99% of the time, you still have the LCL in the knee. It is very rare to have the LCL removed during a knee replacement unless the surgeon saw it was very damaged and would not provide stability to the knee. After a knee replacement, the LCL can be irritated due to a change in your biomechanics post surgery, weakness in the surrounding muscles (especially the quads), and possibly misalignment of the implant. All of these can place excessive stress on the LCL, which can cause pain and irritation.
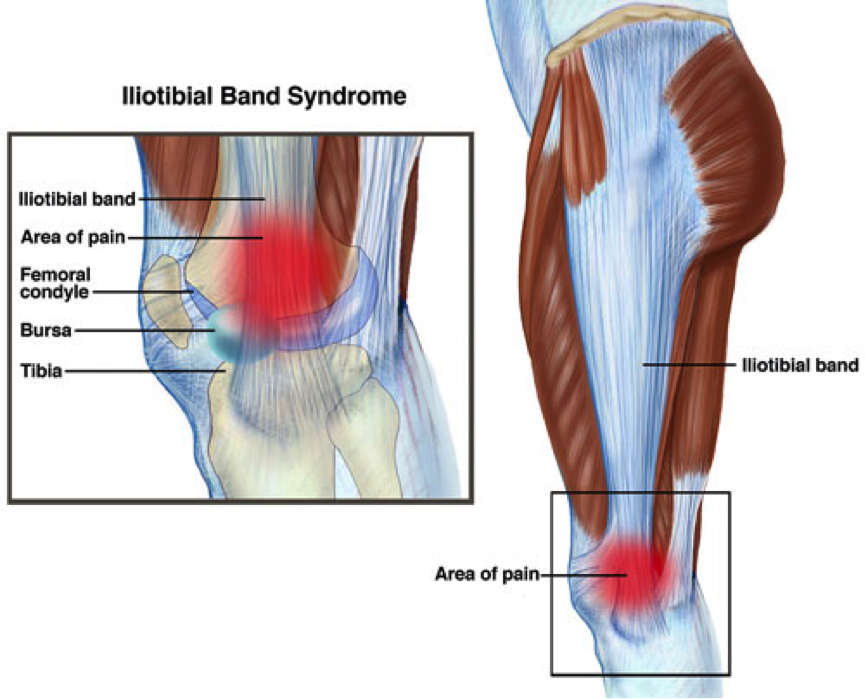
Iliotibial (IT) Band Syndrome
This is one of the most common causes of lateral knee pain in active individuals. When you bend and straighten your knee repetitively (think running or cycling), it causes the IT band to move back and forth over the lateral side of the knee causing irritation from the friction. Another very common cause of IT band pain is from weakness in the glutes, foot and quads. When the surrounding muscles of the knee are weak, the IT band is overstressed leading to more irritation and tension. The IT band is supposed to support the lateral knee. It is not designed to do all the work.
After a knee replacement, weakness and altered biomechanics are the main causes of IT band irritation. Quad weakness is the main muscle group that is weakened after a knee replacement surgery. Although quad weakness is not solely responsible for IT band irritation, it can contribute to other muscles over faciliatating or being overworked in a way they are not designed to. Another important point to make is glute weakness is very common with individual with knee arthritis. Glute weakness is directly linked to IT band irritation. As you can see, general muscle weakness of the leg can be a main cause of IT band problems.
After a knee replacement surgery, the mechanics of the knee also change. The surgeon does change the shape of your knee after surgery so the joint is more neutral. Imagine walking around with the same knee for years and year, and then all of a sudden, after a 2 hour surgery, you wake up with a knee that is completely new shape. All the muscles, tendons, ligaments and soft tissues in the knee, hip, ankle and foot now have to recalibrate or realign to this new shape.
IT band irritation can present as pain along the outside of the knee, tightness of the outside thigh area, snapping when walking or biking.
Lateral Meniscus Injury
The meniscus (medial & lateral) is designed to absorb pressure during walking, standing and other weight bearing activities. If the meniscus was not there, imagine your 2 knee bones (femur and tibia) sitting on top of each other. That would hurt! The meniscus is a key structure in the knee. The meniscus also provides stability to the knee, especially during rotational movements.
When the meniscus is torn, lateral knee pain can occur if the lateral meniscus is affected. Younger individuals usually have traumatic tears, from sports or falls. While older individuals usually experience degenerative changes to the meniscus from repetitive weight bearing and possibly just due to age. Any tears to the meniscus can cause:
- inflammation
- pain with knee motion (especially twisting)
- stiffness in the knee
- catching or locking,
- pain at the lateral joint line
All of these symptoms can lead to further progression of knee osteoarthritis and debilitating dysfunction.
For patients post knee replacement, the lateral meniscus would not be a source of lateral knee pain since the meniscus is removed during a total knee replacement surgery. If you had a medial partial knee replacement, the lateral meniscus would still be intact and could be a source of the pain.
Bicep Femoris Tendon Pathology
The biceps femoris is the outside component of the hamstring muscle. There are 2 parts to the biceps femoris - the short head and the long head. Both heads merge into a tendon that attached on the outside of the knee, more specifically on the fibular head, into the lateral joint capsule and the tissues on the outside of the tibia. This muscle is designed to bend the knee, extend the hip, rotate the tibia (shin bone), and it also stabilizes the outside of the knee. Patients with biceps femoris tendon issues typically report posterolateral knee pain.
This tendon can become irritated over time due to several reasons:
- overuse of the muscles in the legs & not taking rest days
- repetitive knee bending activities like running, hiking, stairs
- poor eccentric control of the hamstrings
- weak surrounding muscles, especially the glutes
- poor walking habits that can overuse the hamstrings
- degenerative changes in the knee joint, which lead to uneven distributions
For individuals after a total knee replacement or partial knee replacement, the bicep femoris can still be an irritant since it is still intact. Because a knee replacement significantly alters the mechanics of the knee, the biceps femoris tendon can become very strained. Small, subtle changes in the alignment of the knee post knee replacement can cause a variety of soft tissue problems.
Scar tissue and adhesions can also restrict movement of this tendon. The tendon is a rope-like structure. It glides back and forth as you bend and straight the knee. If the tendon is being held down by scar tissue, this causes mechanical irritation.
The tendon is also very close to the common peroneal nerve, which is right by the fibular head. Inflammation of the tendon can create irritation of the nerve, which presents as burning, sharp pain, and pains into the lateral/outside lower leg.
Poplietus Tendon
The popliteus muscle is right behind in the knee in the lateral corner. It is very deep in the knee - behind the calf muscles. The purpose of this muscle is rotate the knee. Yes, the knee rotates! It also gives the knee stability in the back of the knee, which is a function of all muscles. When the knee is completely straight, the popleitus locks the femur (thigh bone) into internal rotation. When the knee "unlocks", the poplietus then externally rotates the femur to start the bending of the knee. The popliteus is still in the knee even after a knee replacement.
The poplietus can become irritated or overuse for those who have knee arthritis or weakness of the leg muscles. When you have knee arthritis, sometimes, the knee becomes crooked. You may have a knocked knee formtation (called valgus) or a bow leg formation (called varus). This can create stresses on the poplietus muscle and tendon. It can also cause issues with other muslces and tendons too.
After a knee replacement, the new knee is very different from the old, arthritic knee. There are new tensions on the soft tissues (muscles, ligaments, connective tissue). Some areas that were tight before surgery may now be looser. The joint line may have also changed. The rotational patterns of the tibia and femur also change. That is very shocking to a joint and all the tissues! Tissues do not like sudden changes. Because of the new joint mechanics and changes, the popliteus muscle and tendon can be very irritated.
Symptoms of poplietus tendon pain are:
- deep pain in the back or back corner of the knee
- pain when starting knee bending movement
- pain with stairs in the back of the knee
It can be very challenging to diagnose poplietus muscle and tendon dysfucntion due to its deep position in the knee and confusing symptoms. Overtime, as you become stronger and focus on the appropriate exercises, the muscle should adapt and become less painful.
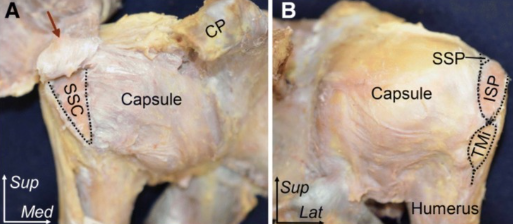
Lateral capsule
All joints have a fibrotic capsule around them. Next time you get a rotisserie chicken, take a look at the joints! You'll see a very thick, white capsule around them. Now, witha human knee, the capsule consists of an outer, middle and deep later. Specifcially focusing on the lateral knee, the outer layer of the capsule (closest to the skin) consists of a thin layer of fibrous tissue and the continuation of the IT band and outer quad muscle called the vastus lateralis. The middle layer of the lateral capstule consists of the LCL and other ligments. The deep layer consists of a membrane that has many pain receptors. The deep layer is responsible for pain in the capsule and scarring.
Joint capsules have a lot of nerve receptors, which makes them sensitive to stretch, trauma, surgery and stress. The inner layer of the capsule can form scar tissue after a knee replacement, which can lead to pain stiffness and pain in the knee.
After a knee replacement, the joint is filled with ongoing swelling and inflammation. Inflammation in the capsule can cause pain, sensitivity and an excessive formation of scar tissue. Some individuals are more prone to scar tissue than others causing the internal/deep layer of the capsule to create thick, dysfunctional tissue.
After a knee replacement, the knee and leg may also be a different shape. Individuals that have malformations of the leg (varus or valgus) may have more adjustments to the tissues after the surgery.




.jpg)




